
Check our patient data records.
Patient Info
- Profile picture

- Last Name
- Parmanad
- First Name
- Shiveena
- Middle Name
- Birthdate
- Age
- Street
- City
- Country
- Zip Code
- Contact number
- 09498851795
- shiveena.p@gmail.com
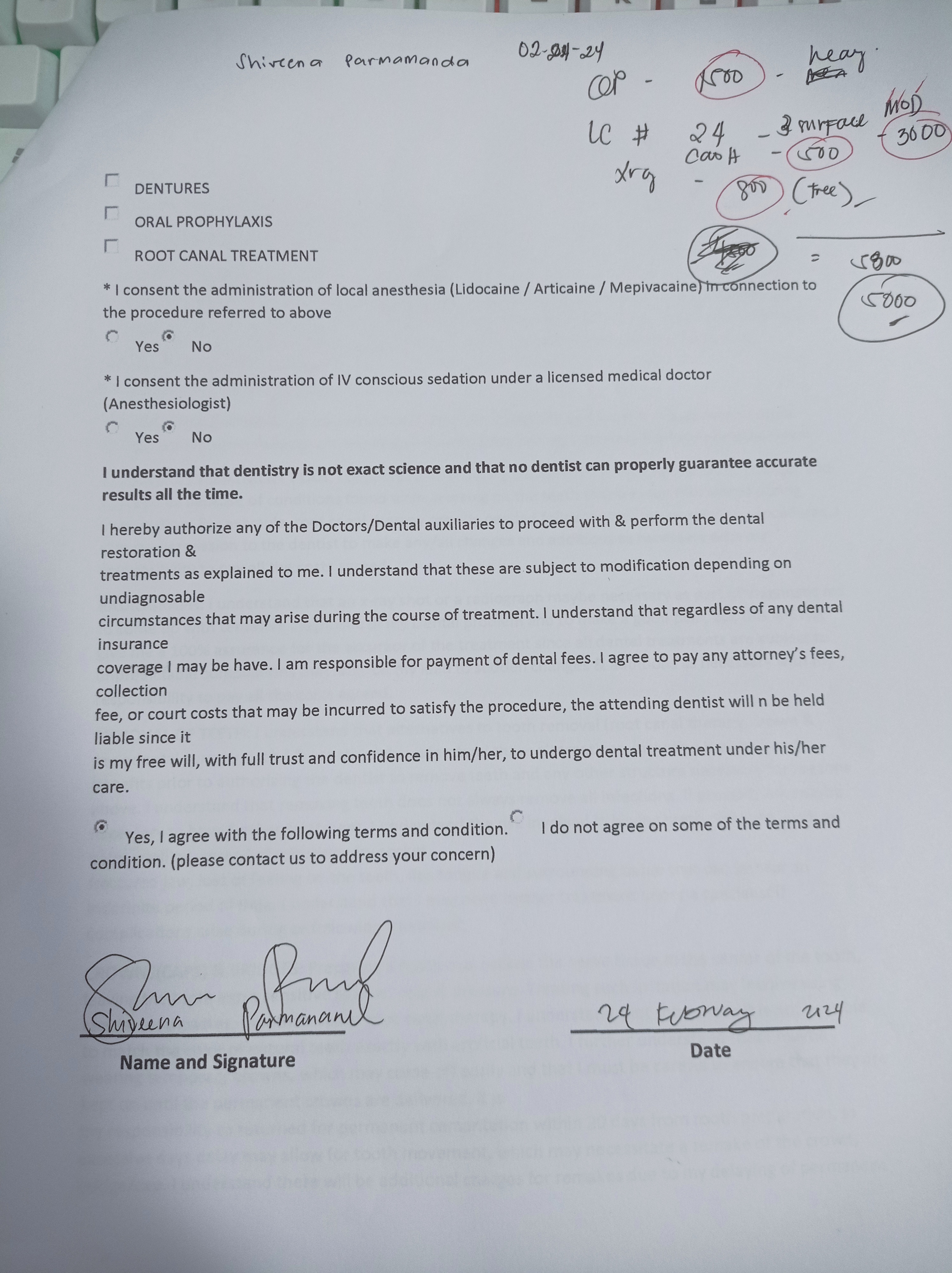
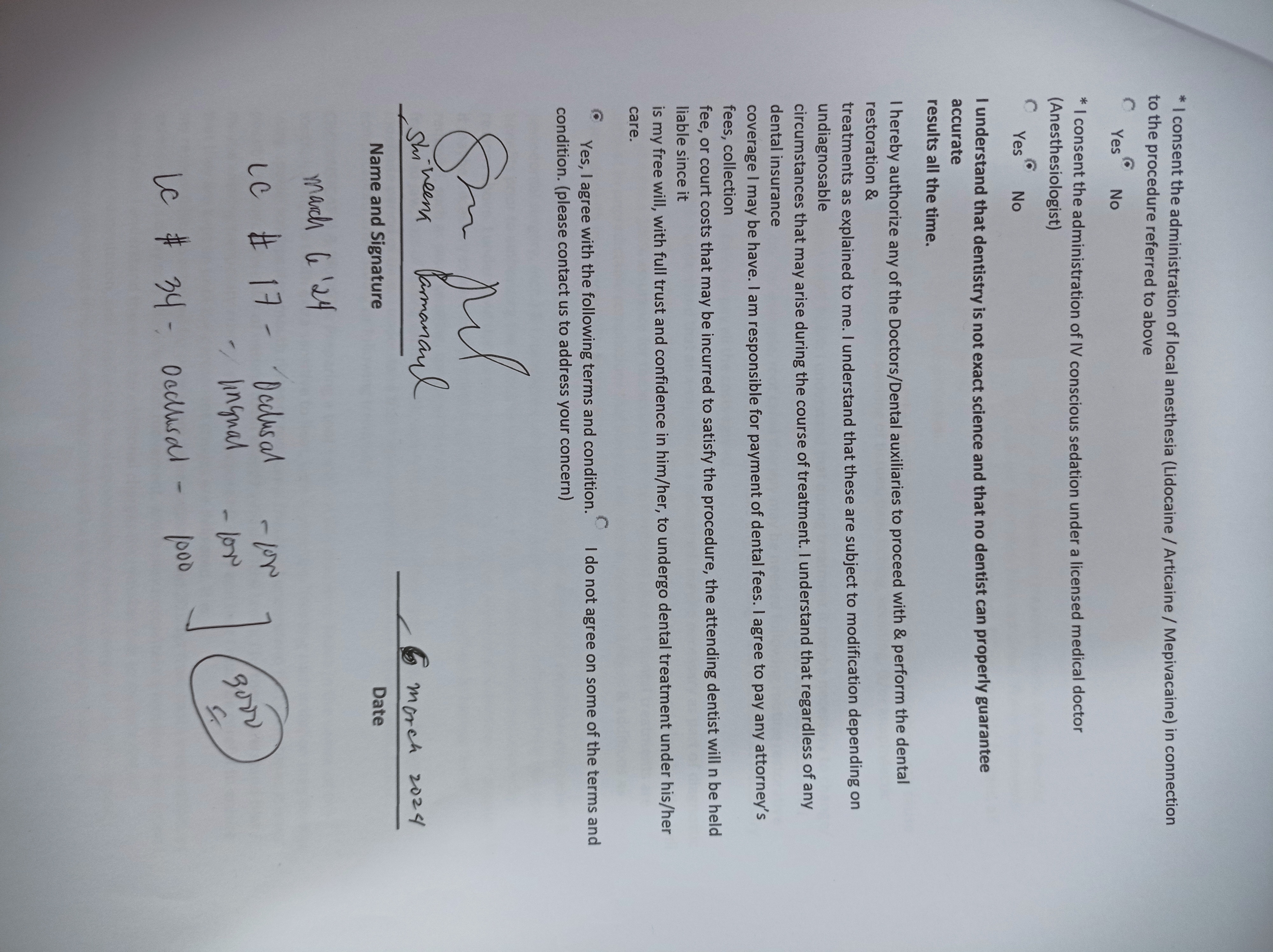
- Procedure
- 02/24/24 OP LC #24-3 surfaces MoD CaOH Xray 03/06/24 -LC #17-occlusal -lingual -LC #34- occlusal 04/17/24 Lc #46 CaoH occlusal distal LC #13 Caoh Distal Lingual facial Xray
{kind=link}
- File 2
- shiveena_parmanad.jpg
{kind=link}
- File 3
- File 4
- File 5
- File 6
- File 7
- File 8
- File 9
- File 10
- File 11
- File 12
- File 13
- File 14
- File 15
- File 16
- File 17
- File 18
- File 19
- File 20
- Retain Record
- Yes